The Role of Early Toxic Interaction with Fathers in Males with Bipolar Spectrum Disorder
Article information

Abstract
Purpose
The etiology of bipolar disorder (BD), a most debilitating mental illness worldwide, focuses on childhood traumatic experiences, some concerning parents. This study explored the role of early toxic interaction with fathers in males with BD.
Methods
This qualitative study used a descriptive phenomenological approach and purposive sampling in Tehran, Iran, in 2022. The data were generated through 12 semi-structured interviews with males with BD who visited psychiatric centers in Tehran, Iran. The interviews continued until data saturation. The collected data were analyzed using Colaizzi’s seven-step method.
Results
The data revealed thirteen subthemes comprising three main themes: the experience of living in constant neglect and rejection, living with fear and abandonment, and reflection of the father’s past interactive patterns in the son’s life.
Conclusion
Living in neglect, fear, and abandonment, and repeating past interactive patterns in current life were some of the bitter life experiences of men with BD, who considered the problematic relationship and misbehavior of their fathers to be somewhat effective in the formation of their life problems, but reported that they could not help themselves with personal and social adaptation. Individual and supportive psychotherapies with drug therapy can help the rehabilitation and recovery of these patients.
INTRODUCTION
Mood disorder, one of the most common chronic and debilitating diseases worldwide, is a brain disorder that causes unusual changes in a person’s mood, energy, and ability to function. This disorder disrupts a person’s performance in relationships, work, and education [1,2]. Mood disorder usually appears in late adolescence or early adulthood [3]. Bipolar disorder (BD; also called manic depression) is a chronic and debilitating disorder, and compared to other mood disorders, has a lower recovery rate and higher mortality rate [3]. According to the World Health Organization (WHO), BD is ranked among the twenty most common disorders in men and women. In the Global Burden of Disease (GBD) report, WHO has identified BD as the sixth most debilitating condition in the world. BD is ranked as the fifth leading cause of disability among individuals aged 15 to 44 years. About 40 million people worldwide were suffering from this disorder until 2019. The Global prevalence of BD was reported to be 0.6 %[4]. In Iran, the rate of bipolar mood disorder was 0.8 % and the frequency of BD among hospitalized patients was reported as 7.9 %[5].
This BD is associated with genetic causes, and brain and environmental changes. However, having an unbalanced, insecure, and toxic parent/primary caregiver interaction with the child is still one of the underlying factors [6]. The early mother-offspring interactions have been specifically explored in research into schizophrenia [7]. Although the theory of schizophrenic mothers has been heavily criticized [8], several studies have shown that the hostile and critical expression of emotions by family members, especially parents, is still one of the causes of the recurrence of mental disorders [9]. The disease may reoccur in patients whose parents or spouses have high levels of criticism, hostility, or emotional conflict during, or shortly after, acute episodes of their illness. The behaviors and attitudes of family members are influential in the formation of the course of mental disorders. Patients with BD who have strong support systems, such as having a spouse who is willing to receive couple therapy, or supportive relatives during hospitalization, have a better course of illness [10-12]. The child’s neglect by the mother as the primary caregiver is more likely to lead to BD in the child [13].
Early parent/child interaction has been considered in classical psychoanalytical theories, until the development of more recent therapeutic models, such as schema therapy. There is a significant relationship between primary maladaptive schemas and BDs [14]. Schemas are formed based on early parent-child experiences, and if these experiences are incompatible and rejecting, they will affect the person’s life and future relationships. Traumatic childhood events are still considered one of the psychosocial causes of mental disorders [15]. Moreover, people who have avoidant attachment and childhood trauma are more likely to commit suicide than others [16]. People who had a traumatic childhood have not been able to form a safe relationship with their parents, while those with avoidant attachment and anxiety are more likely to develop BD in the future [17]. People exposed to emotional maltreatment in childhood are also more likely to develop BD in the future [18]. Research has shown that interpersonal therapy as a treatment complementary to medication prevents the recurrence of BD [19].
Although studies had addressed the primary parent/child interaction, the mother has often been considered the significant parent in early interactions. Mothers as early caregivers play a significant role in the establishment of the child’s behavior [7,8]. Thus, studies have paid less attention to the role of fatherhood in the formation of mental disorders. However, the child-mother relationship has been considered a psycho-social cause of mental disorders experienced by the child. More profound investigations of the father-child interaction go back to the classic psychoanalytic works of Freud and the Oedipus complex [19]. A review of the literature confirms the effects of men suffering from psychological illness and the effects of their illness on the process of fatherhood and parenting [20]. Children of men with mental illness often tend to experience mental disorders in the future. These men have many problems during their transition to fatherhood [21]. Galasiński examined the narratives of fathers with mental illness, and concluded that it is very difficult to be a father and be mentally ill. The fathers loved their fatherhood role, but taking care of and fulfilling fatherly duties was also a difficult task. Galasiński indicated the father-child bounding might directly or indirectly affect the mental health of his offspring [22]. In interviews with male mental patients who were also fathers, another study showed that they loved their role as fathers. However, they were also afraid of losing their children due to their illnesses [23]. Mental illness weakens the image of fatherhood, and fathers worry about the negative impact that mental illness has on their child [24].
However, some studies have addressed the parenting practices used by both parents with an emphasis on the role of the mother [18,25]. For example, a review study showed that mental illness in adulthood is positively associated with patients’ bitter and stressful childhood experiences, childhood experiences relating to emotional and physical neglect, trauma, and victimization, and emotional, physical, and sexual abuse [25]. However, important events and significant others in a person’s life are directly and indirectly related to their current life. Nevertheless, how the experience of living with the father is one of the leading causes of BD needs further investigation.
In addition, when working with patients with BDs in psychiatric centers, the researcher noticed that they had very painful experiences in childhood, especially with fathers who constantly abused and humiliated them. Thus, they could not forget memories of childhood traumas. To this end, this study aimed to investigate the lived experience of these patients with an emphasis on their fatherhood role. This study also sought to discover the role of early toxic interaction with fathers in the formation of BD in males.
METHODS
1. Research Design
This qualitative study was conducted using a descriptive phenomenological design. In phenomenology, the researcher explores the individual life experiences of the participants to discover their concepts and perceptions about life, or the phenomenon in question.
2. Participants
The participants were male patients with bipolar spectrum disorders. All participants were over 20 years old, and were undergoing medication and frequent psychiatric visits. They had a history of hospitalization in psychiatric hospitals in Tehran. The criteria for enrollment in the study were: (1) Having a history of BD for 2 years or more with the diagnosis of a psychiatrist, (2) Not being addicted to drugs or alcohol, (3) Willingness to take voluntary interviews, and (4) Being under medication treatment by a psychiatrist and having stable mental status. After the confirmation of the research protocol by the ethics committee of Khatam University, the researcher conducted interviews with the patients in psychiatric centers.
3. Procedure
At the beginning of the interview sessions, the researcher introduced herself, and provided some information about the objectives of the study. To comply with ethical considerations, the participants were told that their attendance in the interview would be voluntary, and that they could leave the interview if they wished. In addition, written consent was obtained from the participants to record their statements during the interviews. The participants were also assured that their identities would be kept confidential, and that their statements would be quoted using a code, to ensure their anonymity.
The data were collected through semi-structured interviews in line with the objectives of the study. The first participant was 50 years old, single, with a 10-year history of BD, and was under medication. After interviewing the first participant and analyzing his answers, more questions were formulated. During the interview, the researcher provided additional explanations that helped to continue the interview and clarify the issues for the participant. In the end, the participant was asked if he needed to add anything else about the subject matter. The interviews were conducted face-to-face and individually from January 23, 2022, to August 2022. Each interview lasted 45 to 60 minutes, and took a total of 580 minutes. During the interviews and data analysis, the researcher tried to engage in reflexivity by taking notes about the participants’ comments and memos after an interview, and editing her subjective statements. Examples of the interview questions are as follows:
• How was your relationship with your father? What things do you remember from your childhood?
• Did your father’s behavior cause you disappointment and mistrust? How? Can you give an example?
• How did he leave you? Does that mean he didn’t pay attention to you?
4. Data analysis
This study was an applied study in terms of its objectives. It employed a qualitative design and descriptive phenomenological approach for data collection and analysis. To this end, Colaizzi’s seven-step method was used to analyze the data from the interviews, as detailed below [26]. The first step: Familiarity with the data: The researcher read the text of the interviews several times to become familiar with the content of the interviews. The second step: Identifying the significant statements: The researcher highlighted all the significant statements related to the subject under study. The third step: Formulating the themes: The researcher tried to discover the themes underlying the extracted statements, and categorized them to more accurately understand the participant’s statements. The fourth step: Categorizing the themes: The previous steps were performed for all interviews, and the themes extracted from all the interviews were categorized in the form of thematic clusters. The fifth step: Developing a thorough description: The researcher merged all extracted themes to present a thorough description of the phenomenon in question. The sixth step: Developing the core category: The thorough description of the phenomenon was summarized in the form of a core category. The seventh step: Revision: To check whether the thorough description reflected the main themes in the participants’ experience or not, the researcher referred to the participants, and asked for their opinions. If there was any inconsistency, the extracted themes were revised and reformulated.
5. Rigor
To confirm the credibility and adequacy of the findings, the data were revised through member checking by the participants, and peer checking by subject-matter experts. To establish the dependability of the data, an inquiry audit was used, so that the coding and analysis procedures were controlled by the two psychiatric nurses and one psychiatrist. The transferability of the findings was enhanced through the thick description of the context of the study.
RESULTS
Table 1 shows the participants’ demographic data. As can be seen, the participants in this study were 12 male patients suffering from bipolar spectrum disorders. The participants’ age ranged (25 to 51) years.
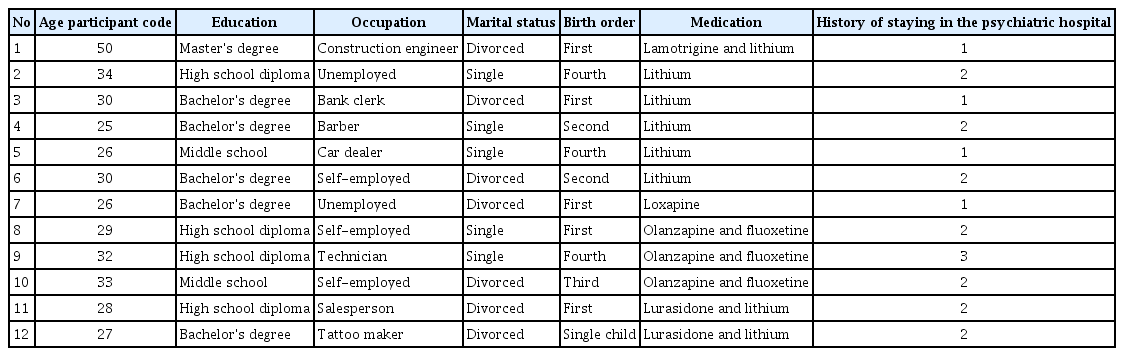
Demographic Data of Participants
The analysis of the data revealed three main themes: “experience of living in constant neglect and rejection”, “living with fear and abandonment”, and “reflection of the father’s past interactive patterns in the son’s life”. Moreover, Table 2 shows the 13 subthemes that were extracted:
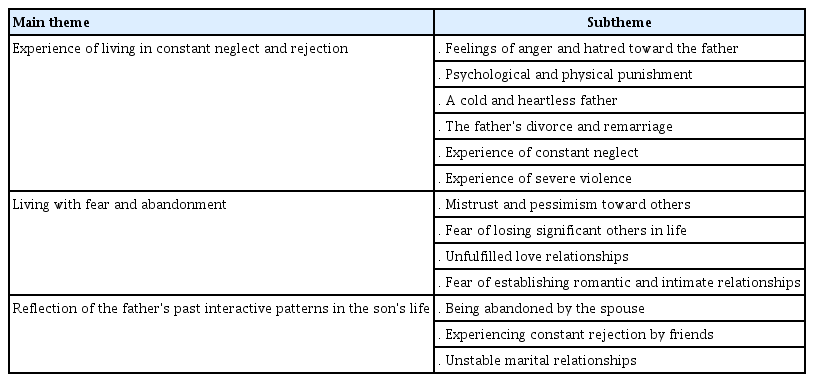
The Main Themes and Subthemes Extracted in the Study
1. The Experience of Living in Constant Neglect and Rejection
The male patients reported that they constantly experienced neglect and rejection in their lives. They stated that they were severely punished by their father, and were constantly humiliated. This theme was subdivided into 6 subthemes, as discussed below:
1) The feeling of anger and hatred toward the father
The participants reported that they had always feelings of anger and hatred toward the father. For example, a participant said,
My father used to beat me all the time for no reason. We lived in a village. When he came to school, I was embarrassed because he would make fun of me in front of my classmates and even beat me. We had a teacher who was a very good man. One day he advised my father that he should not punish his son and it was better to advise him if he made a mistake. Then my father insulted my teacher, and that’s why I was ashamed when I was with other children. I never understood why he treated me so terribly. (Participant #1)
2) Psychological and physical punishment
One of the childhood psychological traumas is abuse and physical harm by the father. As one of the participants pointed out,
I don’t remember my childhood. I mean I don’t want to remember it because I was always beaten by my father, and he used to call me clumsy and a miserable wretch. He always compared the other boys in the family with me and concluded that I was the stupidest of all. He bothered me a lot. I’m still sensitive to loud noises. I think someone wants to punish me. When I grew up, I was enlisted in military service. I had problems in the first few days. Then, a psychiatrist told me that I have a mental disorder and I was discharged from military service. The doctors said I might kill either myself or others. (Participant #2)
3) A cold and heartless father
The lack of affection and support from the father was another theme that was repeatedly pointed out by the participants. Most of them stated that they did not feel any love and intimacy from their father:
My father did not pay attention to me and did not show any affection. He always said that attention and affection for boys spoil them and they should have a manly spirit. That’s why he was very cold toward me. (Participant #5)
Another participant said,
My father was emotionless to me. We lived in a village and in winter there was a lot of snow and the weather was extremely cold. Our village did not have piped water at that time and people had to fetch water from the well, which was very far from our house. Even though my father had a motorbike and was idle at home, he would send me to fetch water and he would not even come himself. Sometimes I hardly fetched water, and my hands were bruised. Then, he would deliberately push me to the ground, pour buckets of water, and then say again, ‘Now bring me back water’. Surprisingly, when he died, I cried a lot, I don't know if my sorrow was for myself or him. Having an insensitive and bad father is a kind of misfortune, not having a bad father does not bring happiness as well. (Participant #1)
4) The father’s divorce and remarriage
Most of the participants were victims of their parent’s divorce, and when they talked about their parents’ divorce and separation, they became nervous and agitated. One of the participants stated:
All my problems in my childhood and adolescence were due to my parent’s divorce. They were constantly quarreling and my father used to beat me. My father suspected my mother and said that she was a prostitute and that she was with other men. But my mother was always at home and was a chaste woman. Once he hit my mother on the head so hard that it started bleeding and my mother ran away from home. She also took me with her but after their divorce, my father said that I should live with him. My father didn’t marry, but he was always with other women and had a mistress. He had nothing to do with me. He was thinking more about himself than me. (Participant #7)
5) The experience of constant neglect
Some participants stated that they were constantly neglected.
Many times, my parents left me alone with my grandmother or relatives. They didn’t even take me to a party or a trip and I knew that they were going on a trip and I wasn’t with them. I felt really lonely and stressed a lot. This feeling of loneliness drove me crazy. I know I had a problem, but what could I do? I once read that loneliness drives people crazy. (Participant #8)
6) Experience of severe violence
Another childhood failure reported by the participants was the father’s beatings and severe physical punishment. One of the participants said,
My father was an addict and constantly smoked drugs or got drunk. He was in his own world. Then he would get angry and beat me and my sister with a belt. My mother also ran away from home because of his beatings. We were alone. He even forgot to feed us. Sometimes the neighbors would take us home and feed us out of pity. After beating us, he would beat himself and pray to God and ask for his forgiveness so that we would forgive him. But the next day he would get drunk again and we had the same story. One day when we were teenagers, my father went out of the house and because he was out of his mind, he was hit by a car and died. They said that he had taken too many drugs and then we went to live with my older aunt. I suffered a lot. My sister takes psychiatric medications like me and is depressed. (Participant #11)
2. Living with Fear and Abandonment
1) Mistrust and pessimism toward others
The participants reported that they were extremely pessimistic about others due to psychological and emotional traumas in their lives. For example, a participant said,
When I was a child, my father was always arguing and fighting with his colleagues at work and he always told me that you should not trust others. He said people are the devil on earth. Later, when I grew up and I would make friends, my father would quickly intervene and said that they were going to deceive me and take advantage of me. He would repeat these words so much that many people would deceive me. (Participant #2)
2) Fear of losing significant others in life
The biggest concern and fear reported by the participants was the fear of losing their loved ones. A participant said,
I never had a good relationship with my father. The only person I love and care for in my life is my mother. Before I separated from my wife, I was always afraid that she would leave me and I strictly controlled my relationship with her. But finally, she left me. (Participant #6)
3) Unfulfilled love relationships
Successive love failures and unfulfilled relationships were among the themes repeatedly pointed out by the participants:
I failed a lot in my relationships with women. I couldn’t have a good relationship with any woman. They left me. They said that I controlled them. All my misery is due to my father’s belief that all women are whores and they are just looking for money. When I met a girl and we got engaged, my father said she was a whore, and when I was not home, she would have sex with other men. That’s why I always suspected her and there were fights until one day my fiance said everything was over. I had the same problem with other women. I didn’t trust them. (Participant #3)
4) Fear of establishing romantic and intimate relationships
The fear of establishing romantic and intimate relationships was another theme that was highlighted by the participants.
My parents, especially my father, were very cold and unemotional. Of course, my father always cheated on my mother and my mother hated him, but she tolerated my father’s misbehavior due to economic problems and her unemployment. Women used to deceive my father and took his money. But my father was happy that he could be with other women all the time. When my brother and I were kids, we would go out in his car, and he would go after other women, and he would always tell us: A man has sexual power and must have relations with many women, that’s how he becomes a man. But you shouldn’t get intimate with these women, and you just have to sleep with them. That’s why when I got older, I only had sex with women and I could not establish romantic relationships with them and I still can’t have a steady relationship with someone. (Participant #7)
3. The Reflection of the Father's Past Interactive Patterns in the Son's Life
1) Being abandoned by the spouse
According to the participants, abandonment by the spouse was the result of constant rejection during childhood by the parents, especially by the father, and repeating the bitter stories of childhood abandonment in adulthood. One of the participants said,
My wife was my enemy. She was the devil herself. She was a very bad woman. She stole all my money and ran away with another man. I told her that I was taking pills and I was sick, but she said I was pretending to be sick. When I was a child, my father always said that I was not sick and I was pretending to be sick to attract their attention. He always told me I was clumsy and I would make them feel disgraceful because I was worthless, even if I got married, my wife would leave me and go with other men. I don’t know why all these terrible things happened to me. (Participant #9)
2) Experiencing constant rejection by friends
The participants in this study reported that they did not have any close and intimate friends, and if they had one at some point in their life, they left them later. A participant said,
I don’t have any close friends, I used to have them, but over time they stopped answering my phone and left me. When I was a child, I used to buy food and gifts for other children to make them friends with me, but then when they took the gifts, they left me. Sometimes I think I am thirsty for love and attention, but there is no one to love me. (Participant #12)
3) Unstable marital relationships
One of the participants said,
My father and mother were always fighting, and my mother often left the house, and after a while, they reconciled and lived together. They were good with each other for a while, but they would start fighting again. My mother said my father was a cold and heartless person and he didn’t pay attention to her at all. When I got married, I got into trouble myself. My wife kept threatening to leave me. After that, she took money from me to stay with me more. In short, we had constant fights and sexual problems. My wife said she was not satisfied when we had sex. Finally, she left me. (Participant #11)
DISCUSSION
The results of the study showed that men with bipolar spectrum disorders experienced three main issues in their interactions with their fathers. They reported living in constant neglect and rejection, living with constant fear and abandonment, and finally the reflection of the father’s past interactive patterns in their life. The childhood of these men - which is ideally the time to form the foundations of personality, create a secure attachment, positive self-concept, and ultimately trust and adapt to the social environment - had passed with the fear of and severe neglect by the father.
Constant neglect and rejection by the father will cause many psychological problems for the child in the future. Pilkington et al. showed that early maladaptive schemas in adulthood are related to a history of childhood abuse and neglect [25]. However, Pilkington et al. only addressed early maladaptive schemas (EMS), but an issue of interest is such schemas are formed in people based on their painful childhood experiences with their caregivers/parents. Thus, the men in this study attributed their current problems to the experience of violence, indifference, and neglect in their interactions with their fathers. Accordingly, their problems were aggravated by anger and hatred towards the father, mental and physical punishment, cold and heartless father, the father’s divorce and remarriage, the experience of constant neglect, and the experience of extreme violence.
Neglect and rejection in childhood are not just related to communication problems in the future. A study showed that there is a relationship between childhood neglect and corticostriatal circuit dysfunction in BD adults [27]. Although physical neglect was addressed in this study, the finding is effective, because we know how neglect can change the brain systems of BD patients. Some of the participants stated that they were physically neglected for a long time by their parents, and there was nobody to meet their basic needs, such as survival needs, nutrition, clothing, shelter, hygiene, and medical care. In some cases, the father even forgot to feed or clean the children.
The participants in this study reported that they were subjected to severe emotional neglect and physical and verbal violence and abuse by their fathers. They were severely punished and humiliated in their childhood. Watson et al. reported a direct relationship between childhood traumas, especially emotional neglect, and BD. These patients have been emotionally neglected more than the nonclinical population [28].
However, an important question is why emotional or physical neglect during childhood can have irreparable effects on people as adults. It seems that humans need to receive attention, love, trust, and be loved by significant others in their lives. When children are exposed to anger, neglect, and abandonment, they do not learn love, trust, and attention. Accordingly, the participants in this study reported that they were living with constant fear and mistrust. They had not been able to experience a stable, trusting, and loving relationship with another person. They had mistrust and pessimism towards others, fear of losing significant others in their lives, unfulfilled love relationships, and fear of establishing romantic and intimate relationships in their lives. In a meta-analysis study, Daruy-Filho et al. concluded that childhood maltreatment is significantly related to the early onset of disorders, suicidality, and substance abuse disorder in patients with BD [29]. The authors stated that childhood abuse, neglect, and maltreatment have a direct relationship with rapid illness progression. In this study, the participants attributed the problematic interactions of their adult lives to verbal abuse and mistrust from their fathers. For example, the father’s hatred of women, or his belief in the child’s inability to establish a permanent relationship with a life partner, was effective in the instability of their marital relationships. In their systematic review, Azorin et al. [30] addressed the impact of BD on couple functioning, and concluded that the negative effects of BD on couples include stigma, lower childbearing rates, sexual problems, and the recurrence of the disease. However, the authors reported positive aspects, such as personal evolution, strengthening relationships, and new hope. The participants in the present study complained about their cold relationship with their partners and sexual problems. Sexual problems were often reported by their wives. The participants also reported that their wives would leave them because of the disease and the stigma caused by it. None of the participants who married had children, as their wives did not like to have children. However, the results reported by Azorin et al. were somehow inconsistent with the findings of the present study [30]. The participants pointed to a positive aspect of the relationship with ex-wives. Of course, this might be because they had divorced their wives and were living alone.
The third main theme in this study was the reflection of the father’s past interactive patterns in the son’s life. The participants reported experiences similar to their fathers’ experience: Abandonment by the spouse, constant rejection by friends, and unstable marital relationships. Before separating from their wives, they had experienced an emotional divorce. The impact of the father's mental health on his child is less considered in the research fields. However, in Fisher's research, the father’s depression indicates the formation of externalizing behaviors in his child [31].
The feeling of rejection and abandonment was also found in male schizophrenic patients. A study examined the early mother-child relationship in schizophrenic patients. The results showed that cold relationships with the mother and lack of care and affection for the child during childhood were reported by patients with schizophrenia [7]. Although this study addressed the relationship between the patient and the mother, the results were significant, because the mother is known as the primary caregiver. Bitter experiences of relationships with caregivers/parents (father/mother) can significantly affect people’s future lives. Relationships that are formed based on neglect, inattention, and the child’s humiliation can cause mental disorders in the future, and make personal and social adjustments of the person difficult.
The present study was significant as it focused on fathers, who are often not taken into account when investigating the underlying causes of psychological disorders. Most studies have considered mothers the main role of caregivers who create secure attachments [7,31].
However, due to the rapid changes in the definition of the family, the existence of single-parent children who usually live with the father, and changes in parenting roles, it is important to pay attention to the role of fatherchild interactions. The participants in this study reported that they were exposed to verbal and physical violence in their childhood. In many cases, they knew that the current toxic interactions were rooted in their childhood. However, they did not know how to get rid of the past, and step toward the future. Thus, mental health professionals need to pay more attention to the father’s role in the formation of early relationships with the child. In addition, the body of knowledge can help in the etiology of bipolar spectrum disorder and the impact of the history of parental and family relationships. Supportive psychotherapy and family therapy, along with medication treatments, can help patients become aware of their problems, and learn how to adapt to their current life.
This study was conducted with some limitations. First, the researcher did not have access to the participants’ fathers, and the participants did not remember the history of their fathers’ mental illness, or did not know if their fathers had a mental disorder. Hence, the genetic causes of BD could not be pinpointed. Second, no participant had a child, while all were separated from their partners. Thus, it was not possible to investigate the effects of this disorder on the family members and children. Thirdly, there is no comprehensive literature on the father’s role in the development or relapse of BD. Although some studies have addressed the relationship between early maladaptive schemas and BDs, they focused mostly on parents, and they often used a correlational design.
CONCLUSION
The present study showed that the toxic and abusive relationship of the father with his child can be reflected in the life experiences of patients with bipolar disorder. These patients often reported the experience of living in constant neglect and rejection, living with fear and abandonment, and the reflection of the father’s past interactive patterns in their life. Thus, early father-child interactions need to receive particular attention in the etiological investigations of BDs. Individual and family psychotherapies, along with medication, can also help the rehabilitation and recovery process of patients with BD.
Notes
The author declared no conflicts of interest.
AUTHOR CONTRIBUTIONS
Conceptualization or/and Methodology: Khodabakhshi-Koolaee A
Data curation or/and Analysis: Khodabakhshi-Koolaee A
Funding acquisition: No Funding
Investigation: Khodabakhshi-Koolaee A
Project administration or/and Supervision: Khodabakhshi-Koolaee A
Resources or/and Software: Khodabakhshi-Koolaee A
Validation: Khodabakhshi-Koolaee A
Visualization: Khodabakhshi-Koolaee A
Writing: original draft or/and review & editing: Khodabakhshi-Koolaee A